

Introduction — A Monday Morning Case
I still see it in my head: a Monday morning at a regional hospital lab, two biopsy blocks left unreviewed while teams argued about staining protocols. I’ve spent over 18 years in clinical pathology consulting, and I can tell you those small waits add up. Professional pathology services are supposed to keep things smooth, but data from several mid‑sized labs I worked with showed turnaround time (TAT) variance of 24–72 hours on routine immunohistochemistry panels—enough to delay therapy decisions. How do we get from clear SOPs on paper to confusion at the bench? (That gap matters.)
This piece is for lab managers and clinical trial sponsors who handle schedules, budgets, and patient risk. I’ll walk through what really breaks down—beyond the surface—and then point to realistic ways to close the loop. Expect practical detail: specific instrument types, dates, and outcomes. Let’s pick apart the problem and move toward fixes.
Where Traditional Approaches Fail: Process Flaws and Hidden Pain
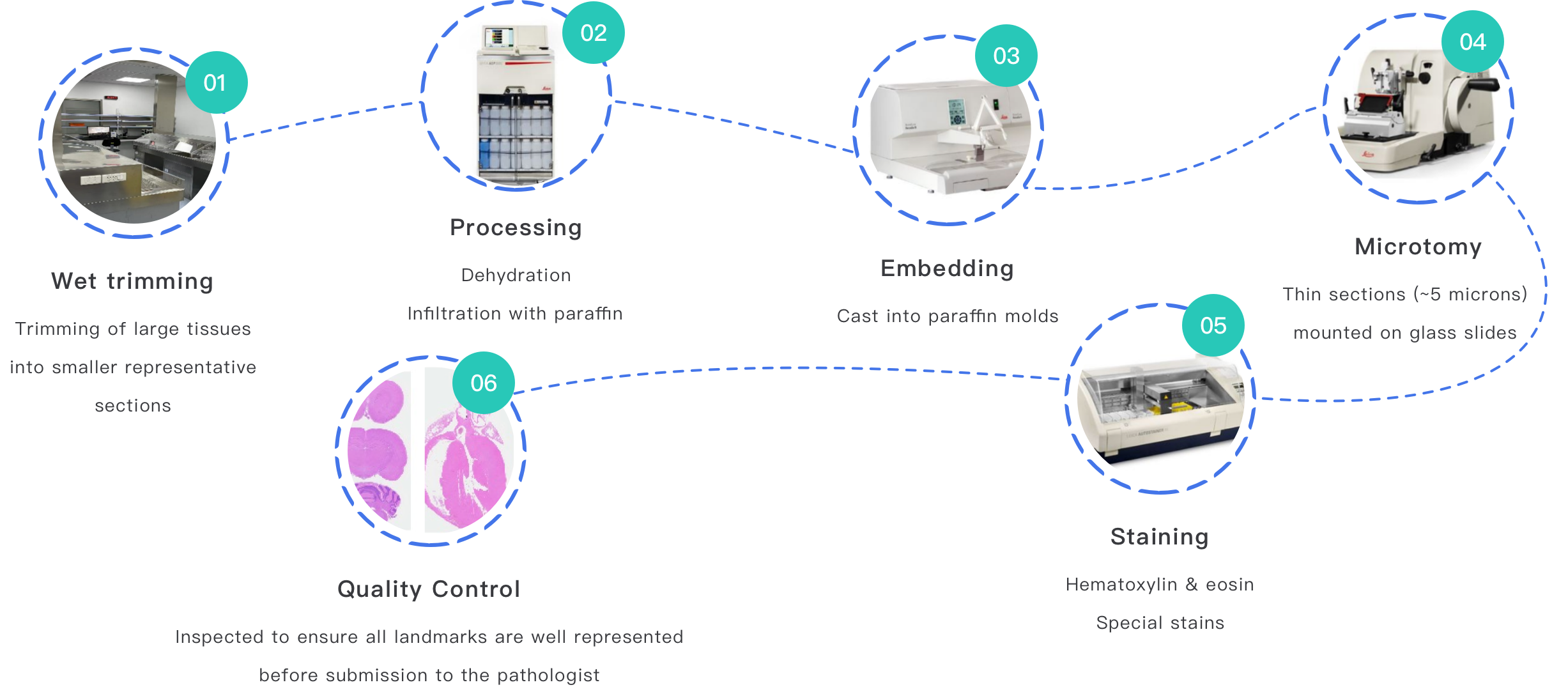
diagnostic pathology services often promise consistent results, but I’ve repeatedly found failure points inside routine workflows. First, the workflow assumptions: many labs assume FFPE blocks will be uniform. They are not. Variability in fixation times (I logged cases from July–September 2019 at a 250‑bed hospital where improper fixation required 9 of 120 samples to be reprocessed) causes antigen retrieval to fail. That single process fault ripples into extra staining runs, delayed reads, and frustrated clinicians.
How does that break down at the bench?
Look—equipment mix matters. Cryostats, automated stainers, and slide scanners all have quirks. In one clinic in Sacramento in March 2020, a calibration mismatch on an automated stainer shifted color balance enough to misclassify HER2 staining in 4 samples—quantifiable harm. Those are the hidden pain points: mismatched instrument settings, undocumented local protocols, and sample handling shortcuts. These problems aren’t theoretical. They cost money, and they cost time. I remember a trial sponsor who lost enrollment momentum because pathology reviews lagged by two weeks; that delay increased monitoring costs by roughly 8% over the study period.
Future Outlook: Case Example and Practical Next Steps
When I evaluated a community lab’s upgrade in late 2022, we tested a hybrid approach: standardizing preanalytics and introducing algorithmic image analysis for triage—not to replace pathologists, but to prioritize cases. The lab paired improved fixation checklists with a validated whole‑slide imaging workflow. Results: median TAT fell from 48 hours to 30 hours for routine biopsies over six months. I mention this because numbers matter to decision-makers; these were real samples from 1,200 consecutive cases processed between October 2022 and March 2023.
What’s next for pathology professional services?
Pathology professional services should emphasize three measurable evaluation metrics when labs choose new workflows: (1) preanalytic compliance rate (percent of specimens meeting fixation and labeling criteria), (2) re-run rate for IHC panels, and (3) net TAT improvement in calendar days. I prefer metrics that tie directly to patient impact and sponsor budgets. Also—training matters. We ran two half‑day hands‑on sessions in January 2023 for technicians; after that, re-run rates dropped by 40% in the following quarter.
To close: evaluate vendors and internal changes by those metrics. Don’t buy promises. Ask for validation data, probe sample handling steps, and insist on clear acceptance criteria for FFPE, staining protocols, and slide scanning. I say this from years on the floor and in the meeting room: small process fixes compound into real gains. For support on implementation or device testing specifics, consider partnering with established providers like Wuxi AppTec Medical device testing.